

Chronic fibrous pulpitis is most often the result of acute pulpitis forms. However, sometimes the primary chronic course of the disease is possible, when the phase of acute inflammation is short-lived and goes away without classical symptoms associated with severe pain.
The chronic form is a kind of compensation when a fibrous degeneration of pulp tissue (“nerve”) occurs with minimal exudation, that is, formation of fluid in the canal. When this occurs, the proliferation of fibrous connective tissue within the channels of the tooth with a corresponding decrease in the sensitivity of the pulp.

Structural changes in the pulp without decay and the formation of pus are the result of the organism's reactivity, when the state of inflammation of the “nerve” tissues makes it possible not to feel acute pain. In most cases, this contributes to tooth decay caries until the pulp chamber, when the outflow of excess fluid from it occurs through the hole in the carious cavity.
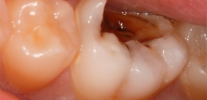
Photograph of a tooth with a deep carious cavity reaching the pulp chamber:

See also article: How caries can look on teeth: photos.
However, in chronic fibrous pulpitis, despite the absence of acute pain, it is not necessary to speak about the welfare of the tooth. Yes, and in most cases this condition is temporary, since sooner or later a part of the pulp can die with phenomena. gangrene "nerve", or necrotization of the entire pulp with the transition of purulent inflammation to the surrounding root tissue.
Acute purulent process, in turn, can spread under the periosteum and cause a "flux", which often leads to tooth extraction. Generally speaking, the transition of the fibrous phase to the pulp gangrene is unpleasant in every sense: a putrid odor appears, the tooth turns gray, strongly reacts to hot, and additional risks of severe complications develop.

That is why it is so important to begin the treatment of fibrous pulpitis as soon as possible, even before the chronic form of the disease becomes acute.
Case history and dynamics of chronic fibrous pulpitis
Chronic fibrous pulpitis among the other forms of pulpitis occurs most often and has a characteristic history of the disease. Usually a person is disturbed by aching pains from various types of irritants (cold and hot food), which do not go away for a long time even after the source of irritation has been eliminated. Often, the pain of the whining character is felt in those cases when the ambient air temperature just changes: for example, when going into a warm room from the cold.
In the presence of deep carious cavity, which communicates with the pulp chamber, pain can not disturb or appear only when chewing hard food due to mechanical irritation of the "nerve". Similar case histories in chronic fibrous pulpitis are observed when the carious cavity is located outside the access to it of irritants, for example, under the gum (root caries).

Why do aching pains predominate in the evening and at night?
Indeed, it is known that toothache manifests itself brighter in the evening and especially at night. Despite the fact that in chronic fibrous pulpitis there are only mild aching pains, but in the evening and at night they often become more intense.
There are several versions about this. According to the first of them, night pains are connected with the fact that during the day a person is active and does not pay attention to weak pain in the background, and in the evening and at night the body relaxes and the pain is felt more acutely. According to another version, the night pains are due to the fact that nerve branches associated with the vagus nerve approach the tooth, and the night has long been called the “kingdom of Vagus”, that is, an increase in the activity of this particular nerve, therefore the tooth hurts more precisely at this time. Dentists, on the other hand, have a closer explanation due to the fact that metabolic processes are weakened in the evening and during sleep, the rate of outflow of toxins from the pulp decreases, which makes its swelling and compression inside the tooth stronger. Since the pulp is a neurovascular bundle, its prolonged compression causes severe pain.
Photo of pulp removed from a tooth:

A case from practice.
A 42-year-old man came to the dentist with complaints about the carious cavity in the upper left tooth, which causes aching pain when eating, as well as a gradual increase in painful sensations from the cold. The patient focused on the violation of the gap between the teeth, because during the meal there is pain in the gums and you have to remove the remnants of food with toothpicks.
From the case history: about a month ago, acute paroxysmal pains appeared in this tooth, which the patient was removing Ketorol painkillers.
Objectively: a deep carious cavity filled with softened and pigmented dentin is determined by visual examination in the left upper fifth tooth (2.5). The medial contact wall and chewing surface of a 2.5 tooth are destroyed by a carious process. When sounding is determined by the point of opening of the cavity of the tooth, which is visible to the pulp. When the probe touches at this point, the pulp bleeds painfully.
To clarify the diagnosis, percussion of the tooth, EDI and radiography were performed. There is no pain during percussion on the tooth, the EDI data is 40 μA On the x-ray there is a message of the cavity with a pulp chamber, changes in the periapical tissues were not detected.
Diagnosis: chronic fibrous pulpitis 2.5 tooth.
Treatment:
- infiltration anesthesia was carried out with SEPTANEST 1: 100 000 (1.7 ml) in the projection of the root tips of the 25 tooth on the gum;
- preparation and machining of the cavity from softened dentin;
- drug treatment with 2% chlorhexidine;
- opening of root canal openings by the fissure bur:
- amputation of coronal pulp;
- extirpation of root pulp by pulpoextractor;
- disclosure of the mouths of the medial and palatal canals by Gates Glidden Pines;
- setting and fixing the working length of the channels;
- the passage and expansion of channels K-files from number 15 to number 40 with alternate drug blasting channels from an endodontic syringe with a 3.25% sodium hypochlorite;
- drying the channels with paper pins;
- channel length control with apex locator;
- canal filling at a given length using cold lateral condensation of gutta percha (No. 35-40, 4 taper) with Endometasone N.
A temporary light-cured Clip is installed on the tooth. The patient is scheduled for the next appointment after 3 days.
Repeated reception. The temporary dressing was removed, the cavity walls were corrected. An open sandwich technique was used: a sectional matrix was set between the 2.4 and 2.5 teeth with wedges to restore the medial contact point.
Vitrebond's glass-ionomer light-cured cement was introduced to the bottom of the enamel-dentin border, the aesthetic-functional properties of the tooth were restored by light-curing Filtek Z-250, grinding and polishing with disks, polishers,brushes with paste Detartrine Z.
The control of the established seal is appointed in a week.
.")
Diagnosis of chronic fibrous pulpitis
The diagnosis of chronic fibrous pulpitis is finally made only after appropriate supporting studies.
Usually, a deep carious cavity is present in the tooth with a softened infected dentin, which often communicates with the pulp chamber. To clarify the presence of such a through message, the dentist uses a probe - a metal instrument that is curved and sharp at the end, which is used for probing.
During this procedure, it is determined whether there is a message from the bottom of the carious cavity to the pulp of the tooth. If there is a message, then after probing the pulp often begins to bleed painfully.

It is interesting
At present, dentists are rarely resorted to for the method of deep probing, or are exercising it with extreme caution. The older generation can tell a lot of stories that an unscrupulous dentist “poked” into the tooth with something sharp during the diagnostics, so that “sparks fell from my eyes”.Such cases, unfortunately, are recorded today, especially at a reception in budget clinics.
Practice shows that severe pain during the sensing procedure occurs when the tip of the probe reaches the bottom of the cavity with excessive pressure. against the background of acute pulpitisrather than chronic. As a rule, in the chronic form, probing an already “injured” food “nerve” does not bring unbearable pain, although modern dentists, taking into account humane diagnostic methods, reject this risky method.
Palpation of the gum near the patient's tooth is always painless, and percussion (tapping) on the pulping tooth with the blunt end of a probe or dental mirror does not bring painful sensations.
One of the important stages of diagnosis is also thermometry - the determination of the tooth's reaction to temperature stimuli. So, for example, if when a cold water is applied to a tooth when it is supplied from a syringe with a blunt needle, the pain does not go away for a long time even after the stimulus has been removed, this indicates a living “nerve” inside the tooth and its chronic inflammation.

As part of the differential diagnosis, electroodontodiagnosis (EDI) is, perhaps,the most informative method, and allows you to accurately determine not only the chronic stage of inflammation with fibrous tissue degeneration inside the tooth, but also to distinguish it from other chronic forms (pulp gangrene and its hypertrophy). Since a healthy pulp begins to respond to a current of 2-6 μA (with deep caries up to 20 μA), all serious deviations from this value indicate a particular state of pulp inflammation. In fibrous pulpitis, the “nerve” responds with excitement and pain with a current of 35-50 μA.
The photo below shows the device for conducting electrical donation diagnostics:

Radiodiagnosis is also important. In chronic fibrous pulpitis on the radiograph of the patient's tooth, you can usually observe a deep carious cavity, which almost always communicates with the pulp chamber. Sometimes there is a slight expansion of the periodontal gap (the space between the root and bone of the alveoli, in which it is fixed).
Differential diagnosis of chronic fibrous pulpitis is performed with deep caries, acute pulpitis and chronic gangrenous pulpitis.It is with these diseases that fibrous pulpitis is most similar.
Deep caries never has a message with the pulp of the tooth, and sounding is painful all over the bottom, and not at one point. The pain quickly passes with the elimination of the irritant, unlike fibrous pulpitis. The indications for EDI in deep caries are no more than 20 μA, and in fibrous pulpitis, from 35 μA.
The acute form of pulpitis is easily confused with chronic. Most of all differences are revealed in the study of the history of the disease, since in chronic fibrous pulpitis there are no complaints of acute spontaneous pain and pain, giving somewhere (in the temple, ear, back of the head, etc.). The patient indicates that there were all these signs earlier, but over time they disappeared and only lasting aching pain remained. When sensing the bottom of the cavity in the background acute pulpitis most often there is no communication of the carious cavity with a “nerve”, unlike fibrous pulpitis.

Gangrenous pulpitis (pulp gangrene) can be confused with fibrous, but its main difference is the appearance of the tooth (grayish tint), putrid odor from the cavity, the destruction of the tooth to the mouth of the canals and pain when probing the channels.Also, the leading indicator in the diagnosis in this case is the data of EDI, which, when pulp gangrene reaches 60 μA.
Surgical treatment of fibrous pulpitis
Since fibrous pulpitis is an irreversible inflammation of the pulp tissue, the treatment involves surgical intervention: partial or complete extraction of the pulp from the canals. You can read about the exciting nuances of this procedure here: How to remove a nerve from a tooth and what problems may arise..

It is interesting
Literary sources of the end of the last century inform that in chronic fibrous pulpitis, a biological (conservative) method of treatment can be applied, but most practicing authors of modern scientific works have concluded that the effect of such treatment is very doubtful, and the forecast for the future is not favorable. Structural changes in the tissues of the pulp do not allow it to return to its former state even at the expense of strong drugs based on antibiotics and calcium hydroxide.
Partial removal of the pulp as a treatment for chronic fibrous pulpitis is extremely rare, since it is difficult to diagnose whether there are serious fibrotic changes in the root pulp.After all, it is the root pulp that, with this method of treatment, preserves and puts on it medicines to relieve inflammation. The complexity of maintaining perfect sterility in the working area and the possibility of re-inflammation of the pulp residues do not allow dentists to hope for success from this type of treatment, and the prospect of redoing work again determines the choice in favor of the method of complete extraction of the pulp from the root canal system.
Complete extraction of the pulp from the root canals reliably relieves the tooth from the source of infection, which provokes pain in the tooth. To do this, use the method of single-stage extraction of the "nerve" with the subsequent cleaning of the channels with antiseptics, or with preliminary devitalization (killing) of the pulp with the help of arsenic paste or arsenic-free analogs.

It is interesting
Due to not the most competent explanations of dentists, the people still believe that after the first visit to the doctor in the treatment of pulpitis in the tooth, a “medicine” is first established. Those who are not lucky with the doctor, this “medicine” also gives severe pain, because in the end it turns out that this arsenic paste was incorrectly installed in the carious cavity and instead of killing the pulp only annoys it.Such a paste does not carry any properties of the drug, of course, in itself, and sometimes in the hands of an inexperienced dentist it becomes poison for the tooth and the organism as a whole.
Modern dentists for the treatment of chronic fibrous pulpitis of any tooth choose the method of complete extraction of pulp from the canals under effective anesthesia. After a good “freezing”, the coronal part of the “nerve” is removed first, and then the root part is removed with the help of pulpoextractors (thin needles, which allow extracting the pulp due to special hooks). After that, the dentist conducts the passage and expansion of the channels with files (tools that have cutting edges and a handle for holding) together with the drug treatment of all the branches of the channel with antiseptic solutions.


Typically, treatment of chronic fibrous pulpitis takes 1-2 visits, depending on the doctor’s tactics. In certain clinical situations, the dentist can put solutions or pastes with strong antiseptics into the canal system to improve the sterilization of the canals and prevent the occurrence of an exacerbation in an already dead tooth, so an additional visit appears.
Features of the treatment of fibrous pulpitis of milk teeth in children
For the treatment of fibrous pulpitis in children today apply different methods, depending on:
- level of dental organization (budget or private);
- clinical case (formed roots or not);
- pediatric dentist professionalism
etc.
Most often for the treatment of fibrous pulpitis of milk teeth with formed roots, a technique is used that is no different from that in adults. The only distinguishing point is that in children, due to the nature of the treatment (excessive activity and fearfulness), paste is often used to pre-devitalize the pulp (usually boneless) to prepare for extraction on the next visit.
")
On a note
For example, Devit-C or - a potent devitalizing paste that does not contain arsenic is used as a devitalizing paste in children. As an active ingredient, it contains paraformaldehyde, which reliably “kills” pulp. For setting this paste with chronic pulpitis in the baby tooth, it is necessary to open the access to the pulp chamber well.Usually, a paste of the size of a millet grain is enough, but for multi-rooted primary teeth the dose is increased individually. Pasta is placed on average for 3-5 days, and sometimes up to one week.
Due to the fact that children most often do not fully carry out all manipulations on canal treatment, which takes a long time to achieve a positive result, pediatric dentists, especially in budgetary clinics, sometimes choose methods of devital amputation, that is, removal of coronary pulp after devitalizing paste and mummification root. Preserving the “dead” root pulp after applying potent mummifying agents is a rather risky undertaking.because the mummified “nerve” can cause chronic inflammation on the root, until fistula occurs on the gum or a cyst on the root of the baby tooth, and this will directly or indirectly affect the germ of the permanent tooth.
Additional information can be found in a separate article: Treatment of pulpitis in milk teeth in children.
From the experience of the dentist
In some dental clinics, resorcin-formalin paste and its analogs in the form of ready-made preparations, which are prohibited in all countries except Russia, are still used as mummifying agents in Russia, except for Russia.The teeth (milk or permanent), cured by this method, look, to put it mildly, not very beautiful: after some time, the entire crown part of the tooth is painted in a shade of pink or red, which is very noticeable to others if the treated tooth is in the smile zone.


Problems that may occur during treatment
During treatment, pulpitis can be both mild and severe complications. Mild complications include those that are easier to correct and that are not so dangerous to human health and life.
For example, the most common mistakes in the treatment of fibrous pulpitis include underpumping of the tooth canals. The quality standard of canal treatment provides for sealing them along the entire length tightly and up to apex - physiological narrowing. If the canal is not sealed to the indicated mark, then in the future there may be big problems associated with the activation of infection in the voids of the canal. It is especially dangerous when the channel is sealed only by 20-50%.


Moreover, dentists are faced with situations where in budgetary (free) dentistry they do not fill canals at all or carry them out with pastes that spread along the walls of the canals, passing off as complete treatment.Naturally, in almost 100% of cases, their colleagues redo work again because of pain or discomfort after improper treatment.
It is most difficult to correct the error associated with the removal of filling intra-channel material beyond the root. Sometimes this mistake is worth the patient's health if the material goes deep into the maxillary sinus (when treating the canals of the upper tooth) or into the mandibular canal (when treating the lower tooth).


In such cases, the removed filling material acts as a foreign body, irritating the tissue and provoking severe pain. Sinusitis develops in the maxillary sinus, and neuritis develops in the mandibular canal. Timely help in the form of surgical intervention by the dentist-surgeon to remove excess material saves health and often the life of the patient. For obvious reasons, a tooth with such a complication often needs to be removed in order to provide better access to foreign material.
Physiotherapy
Physiotherapy treatments for fibrous pulpitis are used both during and after treatment. During canal treatment apply, for example:
- diathermocoagulation "nerve";
- transcanal electrophoresis of iodine.
Diathermocoagulation is the denaturation of the pulp protein or, in other words, its thermal coagulation. Due to the highly heated tip of the needle introduced into the canal, heat is generated, which in a few seconds (2-4 seconds) produces necrosis of the pulp, thereby reducing the risk of bleeding when it is removed. Also, microorganisms are killed, which prevents the penetration of infection beyond the root.
.")
Transcanal electrophoresis of iodine: this method is used in poorly passable channels with a bactericidal purpose, that is, to destroy microbes in hard-to-reach places. This technique allows in the future to avoid the risk of complications such as apical periodontitis - inflammation of the tissues around the root.
If post-filling pain is concerned after the completion of canal treatment, but there are no signs of serious errors in the image that require correction, then anesthetic electrophoresis, ultrasound therapy and laser, as well as microwave radiation, are used. All this allows you to quickly remove the pain of a traumatic nature.
Let's summarize a little.Timely recourse for help with chronic fibrous pulpitis avoids future complications such as gangrene of the “nerve”, followed by its purulent fusion, which means to keep the tooth from being removed. Thanks to modern advances in dentistry, today it is possible to carry out a completely canal treatment with a durable and aesthetic filling. So it makes no sense to endure the pain and drink it with painkillers, it is much easier to cure a tooth and sleep well.
Useful video: what is important to know about pulpitis
Treatment of pulpitis under a microscope
Chronic pulpitis may be the outcome of the acute stage of inflammation of the soft tissues inside the tooth, or an independent disease, but independently ...

The process of necrotization of the pulp tissues (the so-called dental “nerve”) in chronic gangrenous pulpitis is preceded by the stage of its inflammation, ...

Often the teeth begin to hurt at the most inappropriate time - many people are well aware of this the hard way. Often the symptoms are pool ...
My son on a paid admission to the dental clinic was diagnosed with chronic fibrous pulpitis of one of the teeth. On a budget intake, this tooth is indicated as caries. Who to believe?
Hello Olga! Given the paucity of your data, you asked a highly provocative, controversial question. On the one hand, one might think that at the budget intake the complication of caries was negligibly overlooked - fibrous pulpitis, since there is not enough time for detailed diagnostics and there is no desire to bother with several stages of treatment. On the other hand, a paid clinic is often interested in expensive intracanal treatments. Unfortunately, fibrous pulpitis does not always have symptoms, so it is important to see how much the tooth is destroyed and whether there is a message from the carious cavity with the pulp chamber where the “nerve” is located.Sometimes a clue can serve as data on previously occurring sharp pains, which gradually turned into aching and long-lasting. Any information that can confirm a diagnosis is important for further conclusions.